

Introduction: The myeloproliferative neoplasm myelofibrosis (MF) is associated with reduced overall survival (OS) compared to the general population. In 2011, the JAK1/2 inhibitor ruxolitinib, was approved in the USA for the treatment of intermediate and high-risk MF. Long-term follow-up of patients in pivotal phase 3 studies showed survival benefit of ruxolitinib therapy.
Objective: We sought to evaluate the outcome of patients with MF diagnosed before and after the year of 2010 to assess whether OS changed in the past decade in the era of ruxolitinib.
Methods: We retrospectively reviewed the charts of 1346 patients with MF who presented to our institution in the last 25 years and compared clinical parameters and outcomes between those presented before and after the year of 2010 (before / after y. 2010). Newly diagnosed MF patients and patients within 12 months from diagnosis who were previously only treated with supportive therapy (danazol, growth-factors, steroids) were included. Cytogenetics (≥10 metaphases) was classified according to Gangat, JCO, 2011. Molecular analysis (≥ 28 genes) was performed only after y. 2010 by using next generation sequencing platform. Fisher exact test and χ2 were used for analysis of categorical variables. Overall survival (OS) was estimated using the Kaplan-Meier method and comparison was done by the log-rank test.
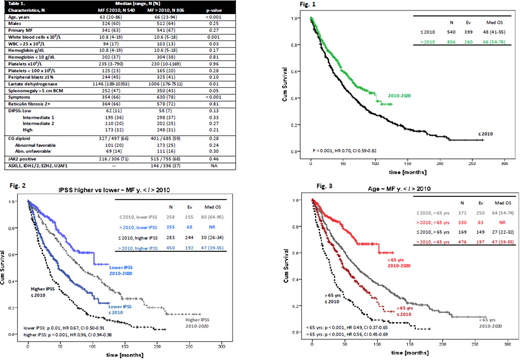
Results: Among the 1346 patients, 806 (60%) patients were seen after y. 2010. Median age of all patients was 65 years (range, 20-94), 62% were males. Patient characteristics with comparison between groups are shown in Table 1. Patients after y. 2010 were older, with lower WBC and lower lactate dehydrogenase, but had more symptoms. The distribution of IPSS scores between groups were comparable at around 10% for low, 36% for intermediate-1, 20-25% for intermediate-2 and ~30% for high risk.
Eighty-five and 80% of patients before and after y. 2010, respectively, received therapy for MF at our institution. Overall, 78 patients (37 after y. 2010) underwent stem cell transplantation. Among treated patients at our institution, 25% (n 117) and 37% (n 241) before and after y. 2010 received ruxolitinib during their follow-up. Ruxolitinib therapy was initiated with a median time of 2 months (range, 0.2-156) from presentation to our institution, longer in those before y. 2010 (11 vs 1 months in patients after y. 2010, respectively, p = 0.001)
After a median follow-up of 30.4 months (range, 0.9-266); 659 (49%) of patients died. More deaths were noticed in those before y. 2010 (74% vs 32 %, respectively, p < 0.001); but these patients had also longer follow-up (37.5 months vs 25 months, p < 0.001). Eighty-five patients (10%) developed acute leukemia: 2 cases per 100 person-years per observation for both groups.
Patients after y. 2010 had superior OS to those before y. 2010 with HR 0.7 (95% CI: 0.59-0.82), p < 0.001, Figure 1. Superior OS was observed in all patients after y. 2010 (vs before y. 2010) when stratified by IPSS score (higher equals for combination of int -2 and high, Figure 2), or age (cutoff of 65 years, Figure 3). Patients exposed to ruxolitinib had superior OS regardless of being diagnosed before or after y. 2010, with respective medians of 98 (95% CI: 78-118) and 91 (95% CI: 73-109) months (details to be presented at the conference).
Conclusion: Our results demonstrate that survival of patients with MF has improved in the last decade. Survival has improved in younger and older patients as well as in those with more advanced disease (per IPSS risks). Many factors may have contributed to the observed improvement in outcome of MF patients, including new therapies, e.g. ruxolitinib, as well as improved supportive management and disease awareness.
Bose:Blueprint Medicines Corporation: Honoraria, Research Funding; Astellas Pharmaceuticals: Research Funding; Kartos Therapeutics: Honoraria, Research Funding; Celgene Corporation: Honoraria, Research Funding; Incyte Corporation: Consultancy, Honoraria, Research Funding, Speakers Bureau; NS Pharma: Research Funding; Constellation Pharmaceuticals: Research Funding; Pfizer, Inc.: Research Funding; CTI BioPharma: Honoraria, Research Funding; Promedior, Inc.: Research Funding. Pemmaraju:Daiichi Sankyo: Research Funding; DAVA Oncology: Honoraria; Blueprint Medicines: Honoraria; Roche Diagnostics: Honoraria; AbbVie: Honoraria, Research Funding; Celgene: Honoraria; Incyte Corporation: Honoraria; MustangBio: Honoraria; Plexxikon: Research Funding; Samus Therapeutics: Research Funding; SagerStrong Foundation: Other: Grant Support; Novartis: Honoraria, Research Funding; Pacylex Pharmaceuticals: Consultancy; Affymetrix: Other: Grant Support, Research Funding; LFB Biotechnologies: Honoraria; Stemline Therapeutics: Honoraria, Research Funding; Cellectis: Research Funding. Kantarjian:Novartis: Research Funding; Ariad: Research Funding; Jazz Pharma: Research Funding; Actinium: Honoraria, Membership on an entity's Board of Directors or advisory committees; Cyclacel: Research Funding; Pfizer: Honoraria, Research Funding; Daiichi-Sankyo: Research Funding; Amgen: Honoraria, Research Funding; Immunogen: Research Funding; Astex: Research Funding; Takeda: Honoraria; Agios: Honoraria, Research Funding; AbbVie: Honoraria, Research Funding; BMS: Research Funding. Verstovsek:CTI Biopharma Corp: Research Funding; Protagonist Therapeutics: Research Funding; PharmaEssentia: Research Funding; ItalPharma: Research Funding; Gilead: Research Funding; Promedior: Research Funding; Novartis: Consultancy, Research Funding; Sierra Oncology: Consultancy, Research Funding; Incyte Corporation: Consultancy, Research Funding; Roche: Research Funding; NS Pharma: Research Funding; Celgene: Consultancy, Research Funding; Blueprint Medicines Corp: Research Funding; Genentech: Research Funding; AstraZeneca: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal